We host one of the largest dedicated collections of systematic reviews on the web, with over 550,000 reviews available. With this vast resource comes a responsibility: ensuring that users critically assess the validity of the systematic reviews they access.
Systematic reviews sit at the top of the evidence pyramid/hierarchy, but their inclusion in this category does not automatically guarantee high-quality evidence. While well-conducted systematic reviews deserve their status, many are poorly executed and risk misleading users.
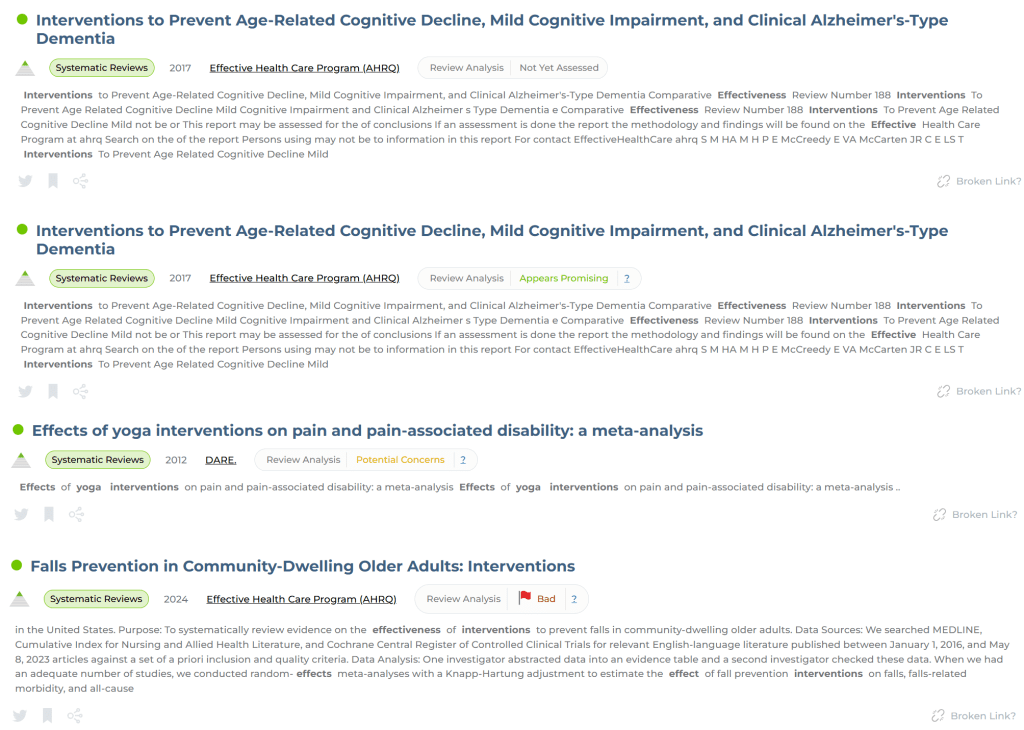
To address this, we are developing a scoring system designed to help users gauge the reliability of systematic reviews. By identifying markers of both rigorous methodology and potential weaknesses, this system will generate a score displayed alongside each review, providing a quick and informed assessment of its credibility. Below is a mock-up of how each score will look:
There are 4 graphics of which 3 are actual, meaningful, scores:
Appears promising
Potential concerns
Bad
We’re working through a few issues but everything is looking promising for a release in the near future (famous last words).
We’ve been having a lot of fun working hard on an automated Q&A system – we’ve been working on and off for over 12 months. Recently we’ve made some big strides and below is an example Q&A. It’s impressive (although I could easily be accused of being biased)!
What is the Role of H. pylori Eradication in Asymptomatic Individuals?
Helicobacter pylori (H. pylori) is a bacterium that infects the stomach lining and is a leading cause of peptic ulcer disease, gastritis, and gastric cancer. While many infected individuals remain asymptomatic, H. pylori is classified as a Group 1 carcinogen by the World Health Organization (WHO) due to its association with gastric cancer. The question of whether to treat asymptomatic individuals is debated, with considerations including the potential to reduce gastric cancer risk and the risks of antibiotic resistance and microbiome disruption.
1. Does Eradication of H. pylori Reduce Gastric Cancer Risk?
Evidence from Meta-Analyses and Clinical Trials:
A meta-analysis of randomized controlled trials found that H. pylori eradication reduced the incidence of gastric cancer by approximately 34% (Ford et al., 2014).
Another systematic review and meta-analysis concluded that individuals who received eradication therapy had a 38% reduction in gastric cancer incidence (Lee et al., 2016).
A cost-effectiveness study using a Markov model showed that a screen-and-treat approach was both effective in preventing gastric cancer and cost-saving in the long term, particularly in high-risk populations (Areia et al., 2013).
Applicability to Western Populations:
Most studies demonstrating the benefits of eradication are from Asian populations, where the background incidence of gastric cancer is high. The applicability to Western populations, where gastric cancer incidence is lower, remains uncertain (Sugano et al., 2015).
2. Are There Official Guidelines Supporting Eradication in Asymptomatic Individuals?
Evidence from Guidelines:
2022 Chinese National Clinical Guideline: Recommends screening and treatment for H. pylori in high-risk populations but does not advocate for universal eradication in asymptomatic individuals (Liu et al., 2022).
Saudi H. pylori Working Group: Provides management recommendations but does not support mass eradication in asymptomatic individuals (Alrashed et al., 2021).
ESPGHAN/NASPGHAN Guidelines: Focus on treatment for children and adolescents with symptoms rather than asymptomatic individuals (Jones et al., 2017).
Targeted “Screen-and-Treat” Strategy:
A study in the U.S. population found that targeted eradication for individuals with a family history of gastric cancer was beneficial (Choi et al., 2018).
3. Are There Risks Associated with Eradication?
Evidence-Based Risks:
Antibiotic Resistance: Rising resistance rates to common H. pylori treatments (e.g., clarithromycin, metronidazole) are a significant concern, particularly in regions with high antibiotic use (Savoldi et al., 2018).
Gastrointestinal Microbiome Disruption: Eradication therapy can alter the gut microbiome, potentially leading to dysbiosis and other gut-related symptoms (Ianiro et al., 2016).
Theoretical Risks:
In low-risk individuals, the benefits of treatment may not outweigh the risks, particularly given the potential for antibiotic resistance and microbiome disruption.
4. Summary and Recommendations
Evidence-Based Recommendations:
H. pylori eradication reduces gastric cancer risk, particularly in high-risk groups (e.g., those with a family history of gastric cancer or living in high-prevalence regions) (Ford et al., 2014).
Screen-and-treat strategies are cost-effective in high-risk populations (Areia et al., 2013).
Guideline Recommendations:
Current guidelines recommend a selective approach rather than mass eradication, particularly in low-risk Western populations (Sugano et al., 2015).
Risks to Consider:
The risks of antibiotic resistance and microbiome disruption must be weighed against the potential benefits of eradication (Savoldi et al., 2018).
Final Recommendation
For asymptomatic individuals, H. pylori eradication should be considered on a case-by-case basis, prioritizing those with gastric cancer risk factors (e.g., family history, high-prevalence areas). Universal eradication is not supported by current guidelines in low-risk populations.
I just had an interesting discussion with a group of NHS librarians from NHS Wales about Trip and the use of LLMs. Most of the features I highlighted were geared towards health professionals, which made me feel a bit guilty about not focusing more on their needs.
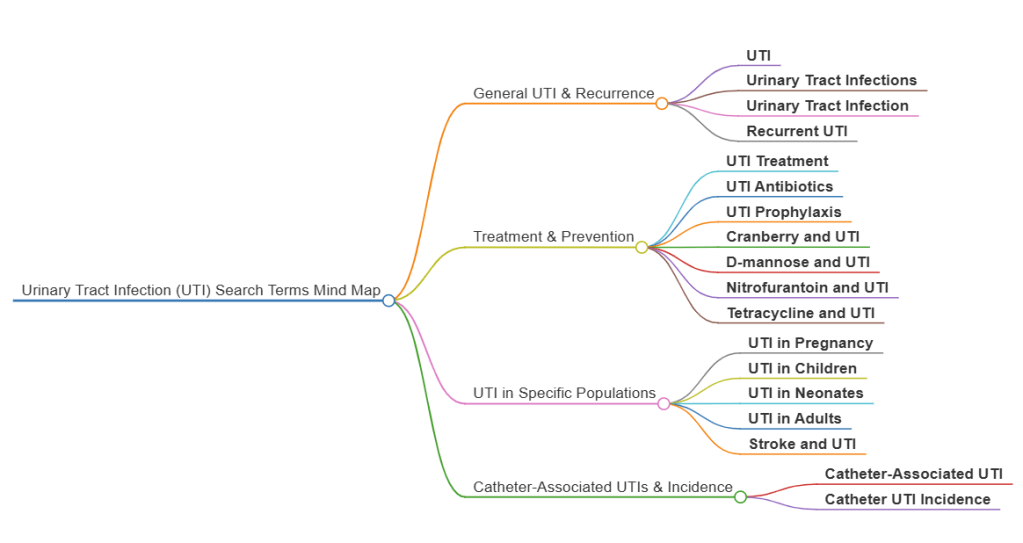
So, at the end of the discussion, I suggested an idea that could benefit a wider audience: using LLMs to analyse past user searches on a given topic and generate related search terms (often a problem for information specialists – identifying additional terms to use in a search). I’ve often thought this could be valuable – essentially harnessing the collective wisdom of our users to improve search experiences.
To test this concept, I took a large list of searches related to urinary tract infections (UTIs) and asked ChatGPT to analyze them. The result? A structured mind map that categorizes searches into key themes, making it easier to explore related topics more effectively:
We’re really excited to announce the launch of our mind map feature, our second AI product (after ‘Latest evidence’)!
A mind map is – according to ChatGPT: A mind map is a visual tool used to organize information, ideas, or concepts in a structured, non-linear way. It starts with a central idea or topic, from which related ideas branch out in a radial fashion. Each branch can have sub-branches, creating a network of connected thoughts. Mind maps help with brainstorming, problem-solving, studying, and planning by making complex information easier to understand and remember. They typically use keywords, colors, and images to enhance creativity and recall.
Seeing an image will better help understand the concept, but to start you need to understand how to create one! Firstly, do a search and at the top of the results you’ll see this:
Note the Mind Map ‘button’ on the right-hand side. You click on that to generate a mind map based on the top 150 search results. In this example we used a search for prostate cancer:
Not only does this give a great topic overview it can support search as each branch and sub-branch is clickable to generate a new search.
This is the fourth in the series exploring how Trip compares with the most popular medical database – PubMed. In relation to a previous comparison we received the following comment recently:
I like this comparison, but I wonder if it would be more meaningful to compare TRIP with a PubMed Clinical Queries search (Clinical Queries – PubMed). I still think TRIP would “win” because of your emphasis on the evidence hierarchy, inclusion of SRs and EB guidelines, but I think it would be a more refined comparison.
ChatGPT describes PubMed Clinical Queries as “…a feature of PubMed designed to help users quickly find evidence-based information relevant to clinical practice. It focuses on filtering search results into predefined categories tailored to specific clinical needs. This tool is especially useful for healthcare professionals seeking high-quality and focused information to aid in patient care.“
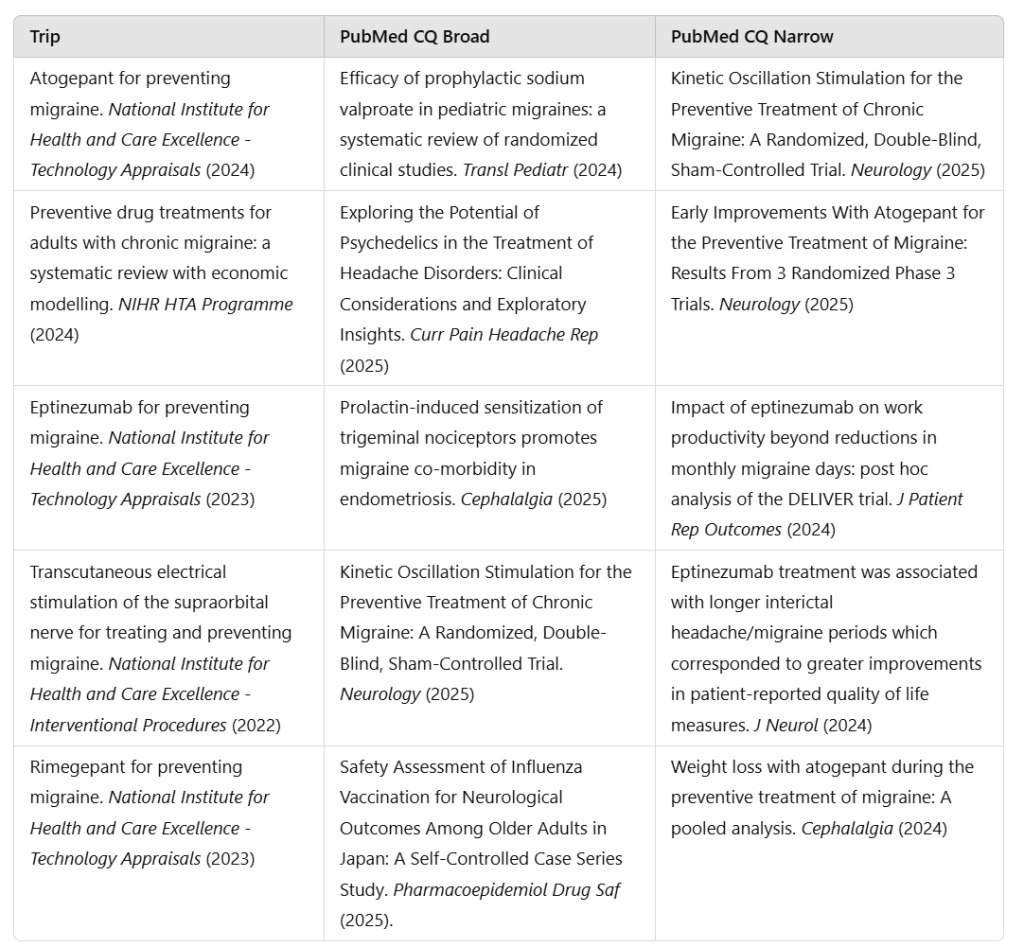
So, sounds like more of a fair challenge, so, lets try it on the search migraine prevention. Clinical Queries (CQ) allows you to select different query types so for this test I selected ‘Therapy’ and after that you have two choices – broad or narrow. Broad maximises sensitivity (trying to identify all possible results) while narrow maximises specificity (trying to identify the most relevant articles). Here are the top five for each database:
To try the search for yourself, here are the links:
For the test I will actually use the top ten results for each database and ask ChatGPT to rate them based on clinical relevance, quality of the evidence and recency. The actual prompt used was:
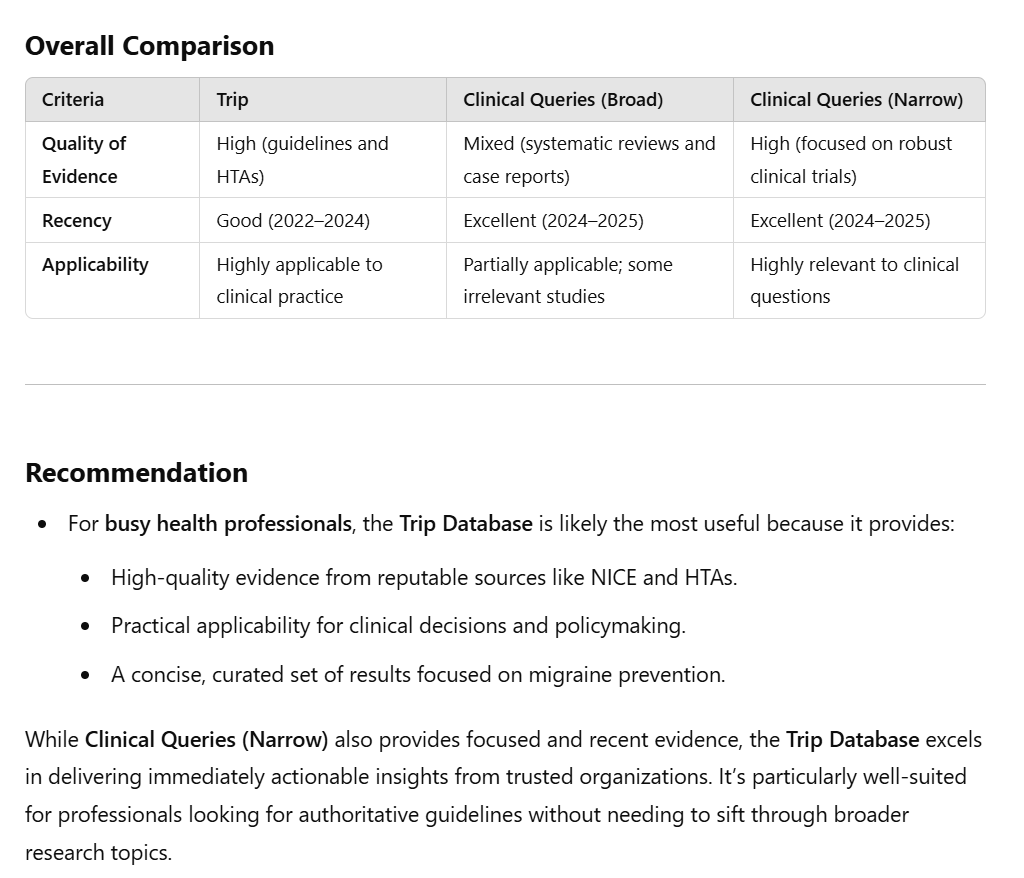
Below are 3 set of results for a search for ‘migraine prevention’. Comment on quality of evidence, recency of articles and applicability to answering questions on the topic. And give an overall view on which database is likely most useful to a busy health professional.
We took a representative clinical question and ran it through Trip Pro, PubMed Best Match (the default algorithm) and PubMed Most Recent. We then exported the top ten results from each – our assumption was that it’s a busy health professional who doesn’t have lots of times to look through pages of results!
The clinical question this time related to the use of use and safety of SSRIs during pregnancy. For each database we used the search terms SSRIs AND pregnancy – you can try the search yourself using these links:
Trip Pro (NOTE: this assumes you have access to Pro)
We then asked ChatGPT to compare the results using this prompt:
Below are three set of results for a search for ‘SSRIs AND pregnancy’ with a view to answering the question about the use and safety of SSRIs during pregnancy. Comment on quality of evidence, recency of articles and applicability to answering the question. And give an overall view on which database is likely most useful to a busy health professional.
It made the following assessment for each database:
Trip Pro: This database provides up-to-date and practical information with fewer older references, making it suitable for answering clinical questions efficiently.
PubMed Best Match: This database offers a mix of high-quality and relevant evidence but includes some outdated material. Its focus on SSRIs in pregnancy makes it useful, but its age range might require careful selection of the most recent and relevant articles.
PubMed Most Recent: This database excels in recency and breadth but may be less practical for quickly answering focused clinical questions due to its diversity and inclusion of less clinically relevant research.
And it gave this final comment:
Recommendation for Busy Health Professionals Trip Pro is likely the most useful due to its balance of recency, applicability, and practicality. It provides high-quality, up-to-date evidence without being overly broad or outdated, making it ideal for answering focused clinical questions about the safety of SSRIs during pregnancy.
We continue to have a impressive impact on care around the globe, helping support millions of decisions with evidence-based content. This is Trip’s core function, as such, it’s ‘business as usual’. However, we have continued to improve the site as much as we can and 2024 was full of significant improvements (BTW this opening section is identical to last year’s review – apart from the update to the year)!
Across the year our Rapid Review (RR) service has brought us great joy and an equal amount of challenge. Doing RRs for sectors we’ve not usually worked with has been particularly interesting. Given our experience and skills we can produce great rapid reviews at a much lower price than most, so if your organisation needs a RR undertaking in 2025, then send us an email: rapidreviews@tripdatabase.com.
January 2024 We spent a lot of time working with LLMs to get to grips with Q&A. Our initial attempts were really encouraging and we know – nearly 12 months later – a lot more of the potential for LLMs.
February 2024 More work on LLMs, this time with a latest evidence feature. This was great fun and is now a live project on Trip (see here), and this is likely to expand in 2025. We also added a large number of new guideline scores to Trip. The title of the announcement Disappointing guideline scores, sums up our thoughts!
March 2024 Many of our searches are really simple so it was great to better understand the motivations of our users with by launching a survey. We also had a blast from the past, courtesy of the Internet Archive, with the original 25 publishers included in Trip:
August 2024 A quiet month with a simple announcement regarding miss-spelling!
September 2024 We released the mis-spelling feature mentioned above but more importantly we broke a record for the number of systematic reviews we link to, with over 550,000!
October 2024 Latest evidence was launched! This is going down really well and so we’re looking to expand to areas outside of primary care.
November 2024 Trip is often asked how to we compare with PubMed. To help we created a comparison based on an example search. We have now done two comparisons (one and two). We used ChatGPT to undertake the analysis – felt it was less biased than asking ourselves. If you’re interested in answering clinical questions using high-quality evidence then the results are clear….
December 2024 We released some important design changes (see here and here). Many were small but boosted transparency and usability of the site.
We also started working with Mind Maps, really amazing feature that we hope to roll out in early 2025. This combines LLMs and a lovely graphical interface.
If we had to summarise 2024 it would be the year we got comfortable with LLMs (as you’ll see in 2025) and the year we continued to push out new features to make Trip a better service for our users. And, in the spirit of this year and next, we asked ChatGPT to summarise our year:
In 2024, Trip Database focused on leveraging LLMs for innovation, enhancing infrastructure and usability, and expanding evidence-based features like “latest evidence.” User feedback and AI played central roles in refining offerings, while milestone achievements and transparency-driven updates set the foundation for future advancements.





Recent Comments