These last few months have been hard work!
- Mid-March we released the Controlled trials filter in Trip. 500,000 trials, all easily searchable and incorporated into Trip.
- Also in mid-March I presented at EvidenceLive 2013, where I gave a talk under the interesting title ‘Anarchism, Punk and EBM’. The broad thrust can be read in my A critique of the Cochrane Collaboration blog article. This has now been read nearly 4,000 times.
- In early April I set about recruiting for the new Trip Advisory Board. It’s a 20 strong group of clinicians and information specialists from around the world. This group will become active in the near future and will help advise me on the way forward for Trip.
- I had some good fun creating the Trip Pinterest account. I view this as a simple way of posting pictures which I can easily link to!
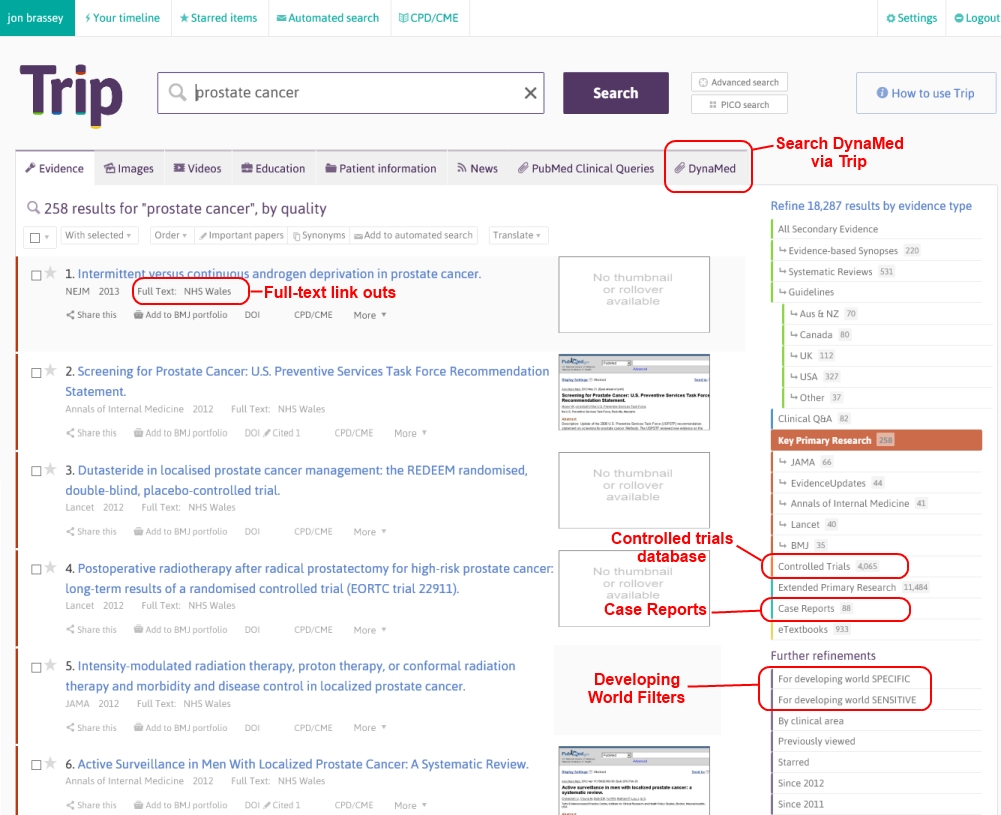
- More recently I have been concentrating on the latest upgrade to Trip. The highlights being better access to full-text articles, a ‘developing world’ filter, integration of DynaMed and case reports and a host of other minor changes. The full-text feature is a personal triumph as it has taken me so long to figure out how it’s done! Successive surveys have shown better full-text access as a priority so, finally, to be able to help is wonderful. As I write this, we have 199 institutions signed up and over 350 individuals have aligned themselves with their institution – not bad for 3(ish) days. Currently, individuals from Barts Health NHS Trust, NHS Scotland, King’s College London, Academisch Medisch Centrum and University of British Columbia are the biggest institutional ‘subscribers’
- We’re often asked about promotional material and we’re very close to getting some leaflets produced. On our Pinterest account you can see the final designs.
Not a bad two months for Trip.
But, there’s no resting and other plans are taking shape:
- Clinician similarity is something I blogged about in 2012. Fairly quietly I’ve been working quite hard on this and have recently received funding to work with the University of Glasgow. We’re hoping to have initial results of that in the next 2-3 months.
- Reporting even earlier than that will be another project I’ve been working on – near instant reviews. Trip funded phase one and we received a grant to work on phase two. This is really exciting as the phase one results were so promising. At the end of this phase we should have a tool for people to experiment with. The principles are sound, the technology looks good but I can’t help feeling acceptance will be the hard part!
The above are the two main projects I’m working on. But that leaves future projects and this is where the advisory board will help. A few example projects that I’m keen to explore:
- Patient interface – very excited by this
- Mobile interface
- Better publicity
- Creating of a decent business model, which may include a freemium Trip
- Improved full-text access, improve our initial offering
- Further improve the timeline experience
- And a handful more speculative/spectacular ideas
Happy days!

Recent Comments