Trip has been operating for over 15 years and I can easily say we have arrived at the most significant breakthrough yet. It is still in our ‘labs’ section and still has much work to do before being rolled out. But, the path is clear and, finance aside, there is no reason why we can’t produce a significant increase in search performance.
In search a really important concept is intention. So, when a user searches they may add 2-3 search terms but what are they thinking about when they use those terms? For instance, and this is a true story, I showed Trip to a Professor of Anaesthesiology and asked for his views on the site. He came back saying that he was unimpressed! The reason – his interest was in awareness (as in, when a person is under anaesthetic are they truly anaesthetised or may they be aware) and when you search Trip for awareness you get lots of results, mostly on things like the awareness of public health messages! Another example I use to illustrate the point is the search pain. We return the same results whether the person is an oncologist or a rheumatologist – which to me is ridiculous – as the intention is likely to be significantly different. But, to date, there has been no good solution.
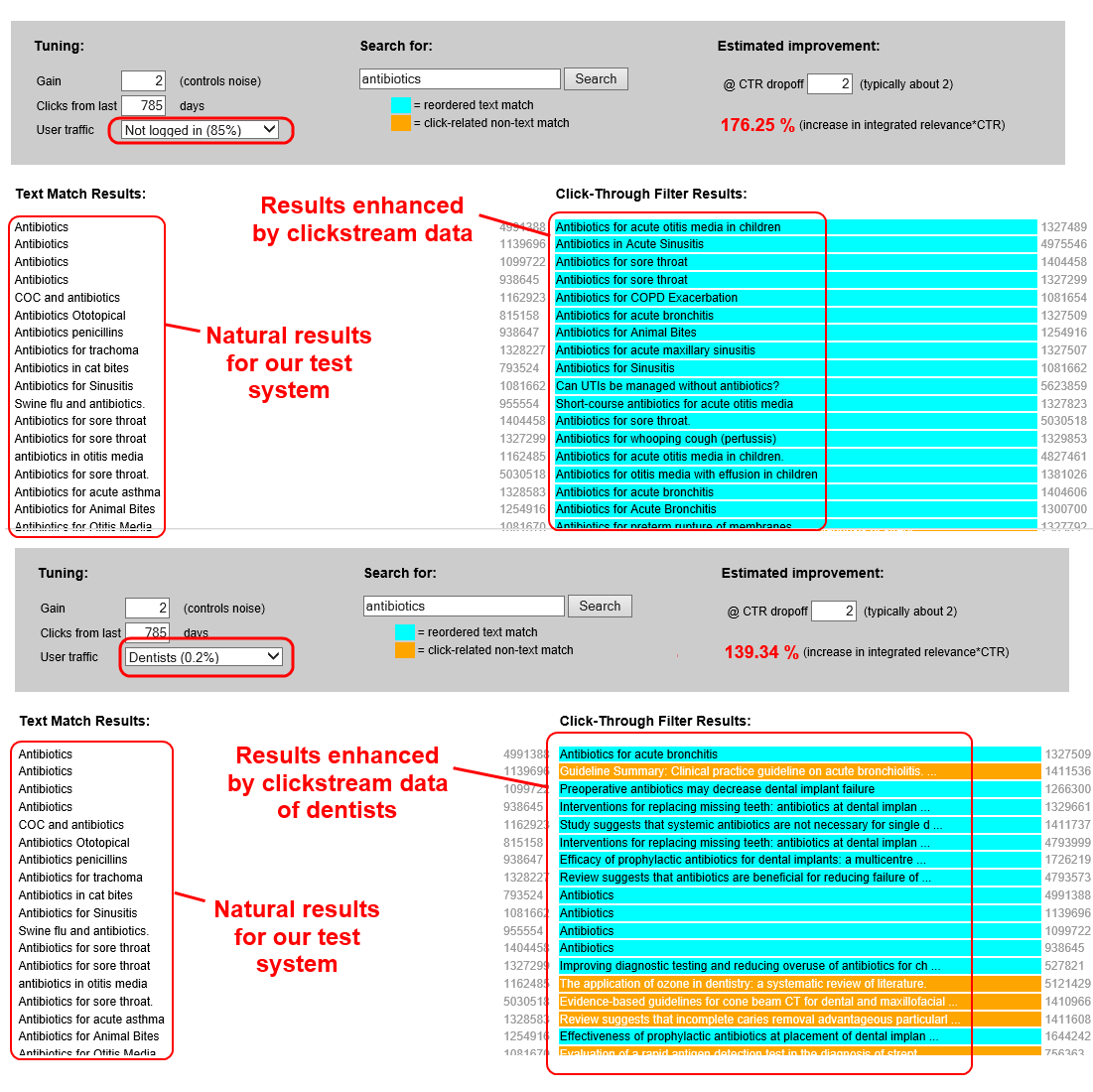
The below image (click to enlarge) shows a breakthrough.
In the image above there are 4 sets of results for the same search antibiotics. This is a test system and not based on the real Trip results. However, on the left-hand side we have the normal/natural results for the search antibiotics in the test system. In the top right set of results the natural results have been reordered based on the clickstream activity of the users of Trip, those who have not logged in (85%). At the simplest level this promotes results that have been clicked on and relegates those that have not been clicked. It really is more complex than that – but I hope you get the point!
But the bottom right is where the magic it. Even though it only accounts for 0.2% of the activity, we have reordered the results based on the clickthrough activity of dentists. There are a few erroneous results, but I’d like to think you can see the effect – dental articles are promoted.
So, the effect of this is that – when we eventually roll out the system – and we know the user is a dentist we improve their results based on the previous activity of other dentists. The reality is that this technique will work with any speciality and profession.
There are a few issues, the paucity of data is the biggest and we have two significant ways of tackling this:
- When we roll out the new Trip we will – to a large extent – make login/registration obligatory. This will mean we get lots more clickstream data which will make the results even better.
- Machine learning. We’ve already worked on machine learning and will bring these techniques to the system to enhance/compliment the clickstream work.
Oh yes, we’ve even figured out a way to mitigate the effects of filter bubbles.
This really has been a good few weeks.

Recent Comments