2024 was a great year for Trip.
We continue to have a impressive impact on care around the globe, helping support millions of decisions with evidence-based content. This is Trip’s core function, as such, it’s ‘business as usual’. However, we have continued to improve the site as much as we can and 2024 was full of significant improvements (BTW this opening section is identical to last year’s review – apart from the update to the year)!
Across the year our Rapid Review (RR) service has brought us great joy and an equal amount of challenge. Doing RRs for sectors we’ve not usually worked with has been particularly interesting. Given our experience and skills we can produce great rapid reviews at a much lower price than most, so if your organisation needs a RR undertaking in 2025, then send us an email: rapidreviews@tripdatabase.com.
January 2024
We spent a lot of time working with LLMs to get to grips with Q&A. Our initial attempts were really encouraging and we know – nearly 12 months later – a lot more of the potential for LLMs.
February 2024
More work on LLMs, this time with a latest evidence feature. This was great fun and is now a live project on Trip (see here), and this is likely to expand in 2025.
We also added a large number of new guideline scores to Trip. The title of the announcement Disappointing guideline scores, sums up our thoughts!
March 2024
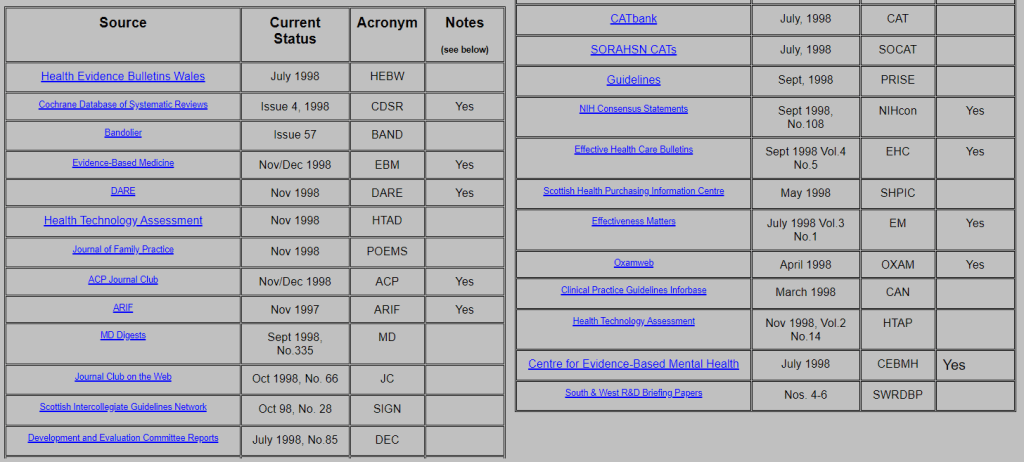
Many of our searches are really simple so it was great to better understand the motivations of our users with by launching a survey. We also had a blast from the past, courtesy of the Internet Archive, with the original 25 publishers included in Trip:
April 2024
More fun with LLMs including extracting recommendations from guidelines and systematic reviews and using them to analyse clickstream data.
May 2024
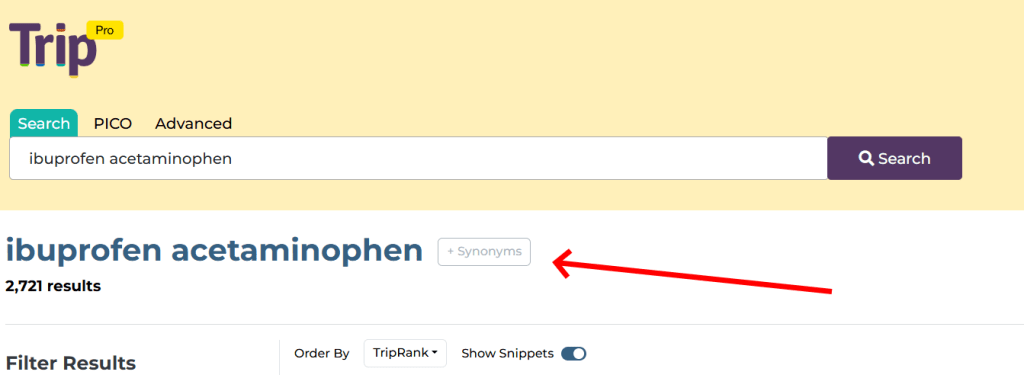
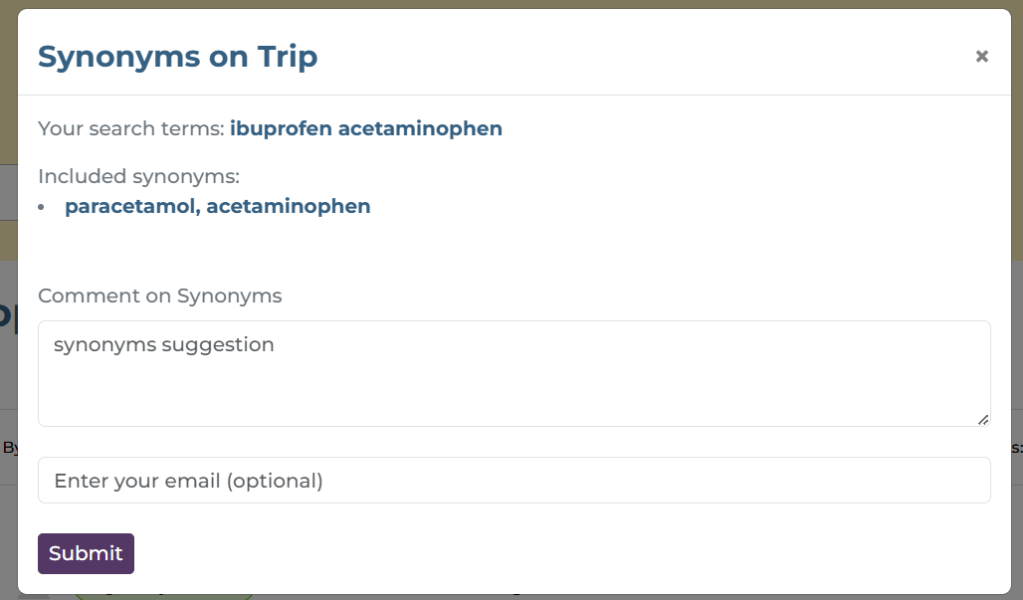
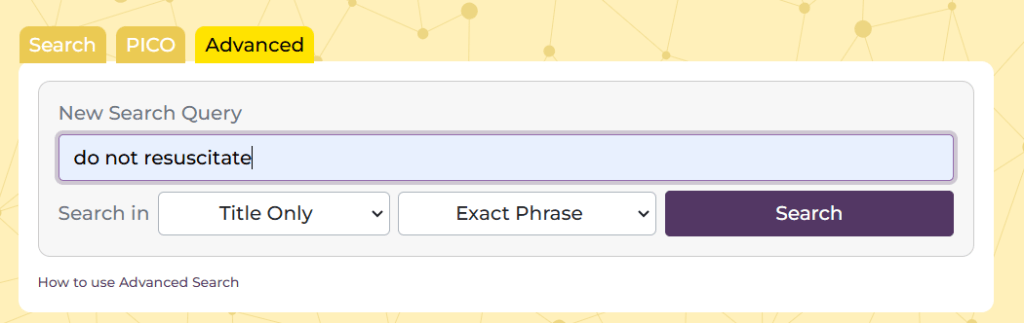
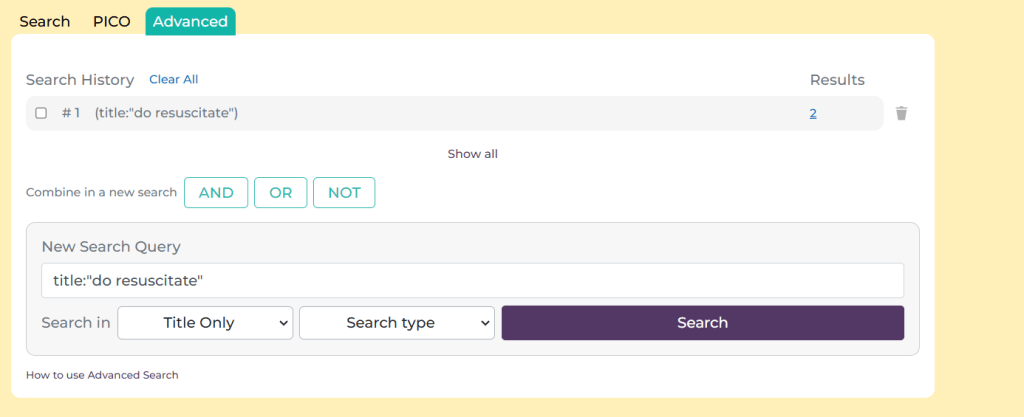
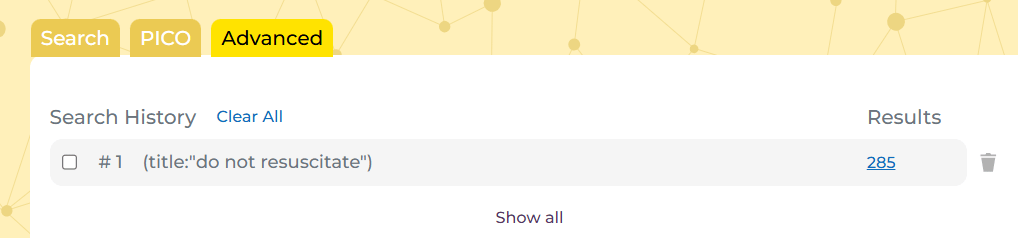
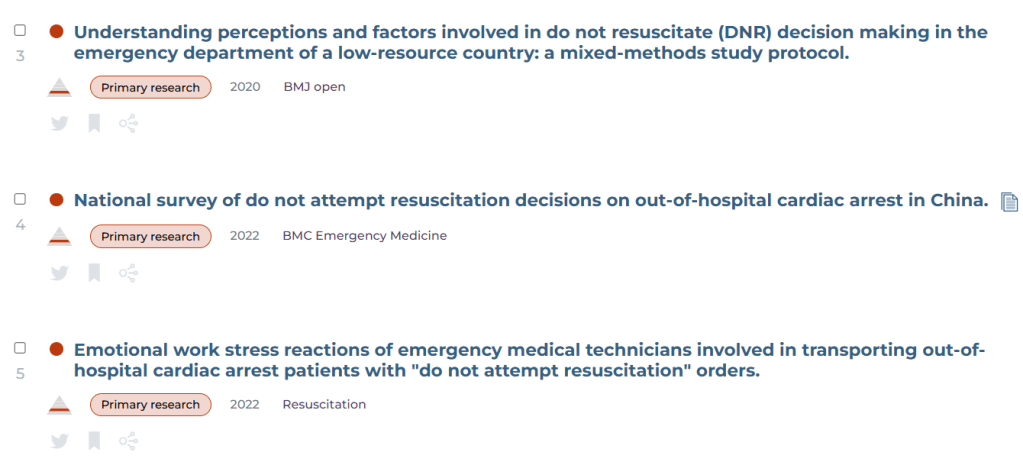
This was a really significant month. We moved our infrastructure onto the cloud and made a really big change to our search results.
June 2024
Another user survey, this time asking our users about their thoughts on our use of AI.
July 2024
As well as releasing the results on the AI survey we improved our inclusion of full-text documents (for Pro users) with over 85% of our journal articles linking to full-text.
August 2024
A quiet month with a simple announcement regarding miss-spelling!
September 2024
We released the mis-spelling feature mentioned above but more importantly we broke a record for the number of systematic reviews we link to, with over 550,000!
October 2024
Latest evidence was launched! This is going down really well and so we’re looking to expand to areas outside of primary care.
November 2024
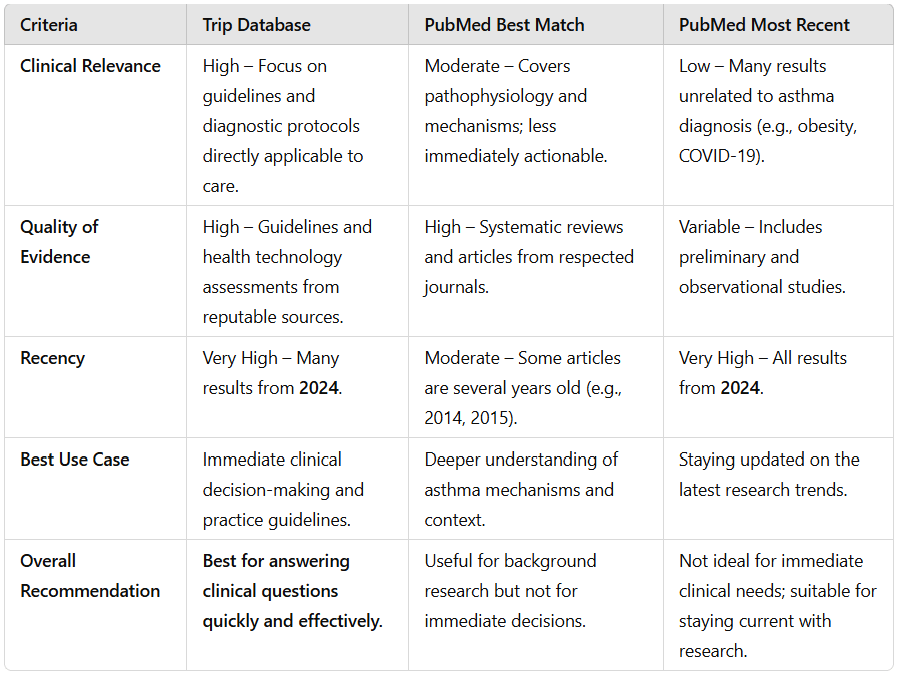
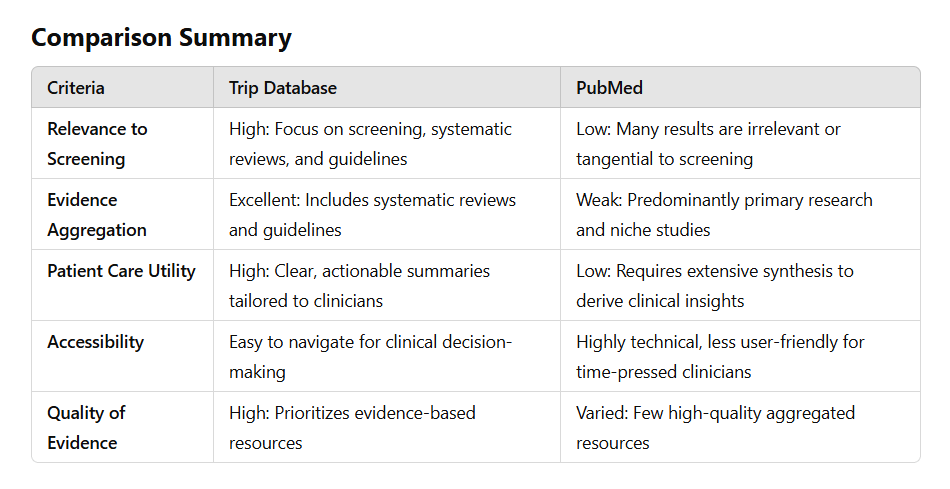
Trip is often asked how to we compare with PubMed. To help we created a comparison based on an example search. We have now done two comparisons (one and two). We used ChatGPT to undertake the analysis – felt it was less biased than asking ourselves. If you’re interested in answering clinical questions using high-quality evidence then the results are clear….
December 2024
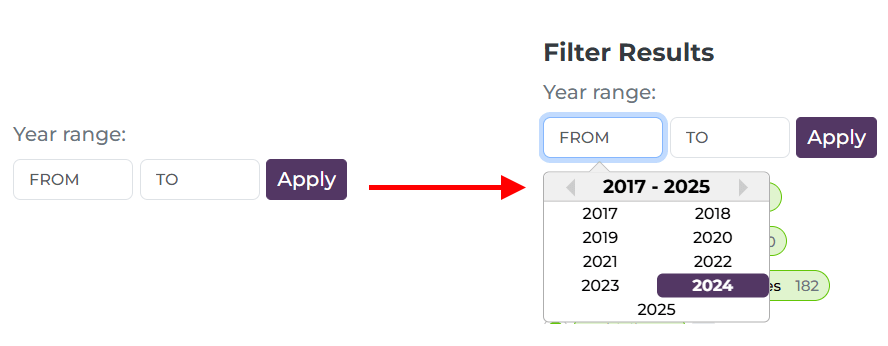
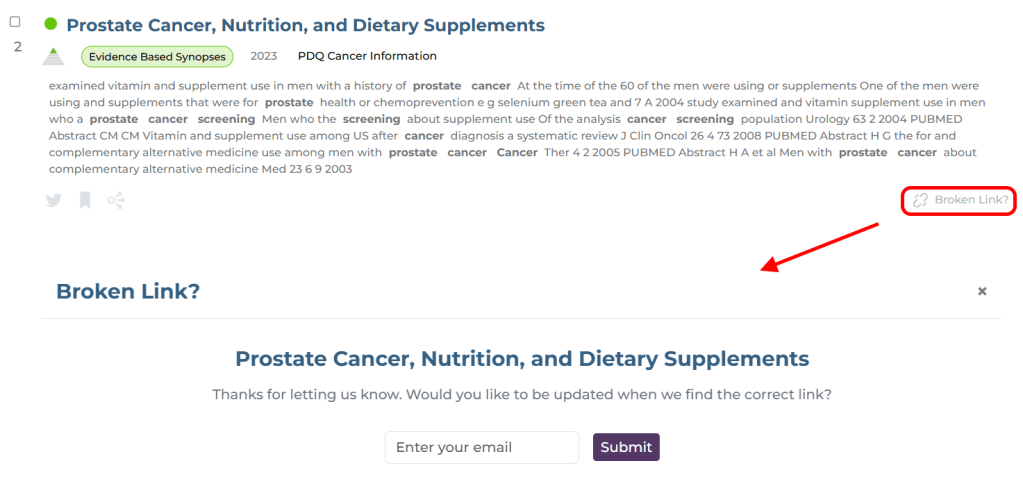
We released some important design changes (see here and here). Many were small but boosted transparency and usability of the site.
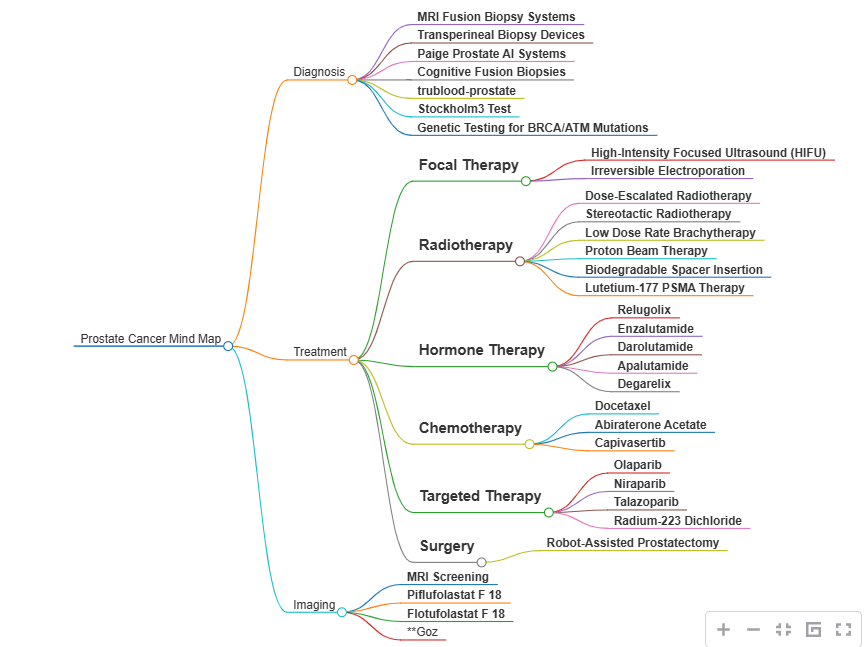
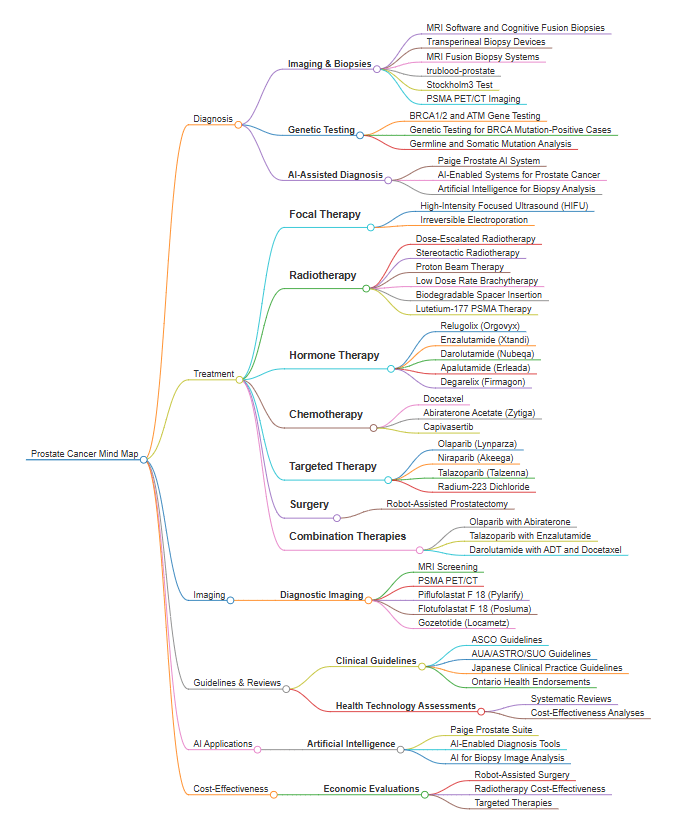
We also started working with Mind Maps, really amazing feature that we hope to roll out in early 2025. This combines LLMs and a lovely graphical interface.
If we had to summarise 2024 it would be the year we got comfortable with LLMs (as you’ll see in 2025) and the year we continued to push out new features to make Trip a better service for our users. And, in the spirit of this year and next, we asked ChatGPT to summarise our year:
In 2024, Trip Database focused on leveraging LLMs for innovation, enhancing infrastructure and usability, and expanding evidence-based features like “latest evidence.” User feedback and AI played central roles in refining offerings, while milestone achievements and transparency-driven updates set the foundation for future advancements.


Recent Comments