I had a great meeting with Carl Heneghan at the Centre for Evidence Based Medicine yesterday. I went with an agenda which Carl skillfully dispatched and then turned everything on it’s head. I believe I’ve recovered.
One issue we touched upon was new research and how to keep up to date with the latest evidence. At Trip we aggregate the World’s evidence. If there’s new high-quality research it should be (and probably is) in Trip. But Trip is a search engine.
Chris (my partner in Trip) is a GP and he uses Trip to answer clinical questions. To him this is what he wants Trip to do and he’s very happy with how it works.
Carl, on the other hand, wants to know what’s new and what to take notice of (as well as searching for answers).
So, what can we do to help? We have our monthly emails, but they’re far from perfect. There are oftern way too many results (especially in primary research). So, one potential approach is to just highlight new research from the categories of secondary evidence (systematic reviews, synopses and guidelines) and key primary research (big 5 internal medicine journals plus the output from ‘EvidenceUpdates’). If we take the example of diabetes, below is the complete list (from last month) of articles with diabetes in the title (an important distinction) from the ‘top’ sources:
- Different intensities of glycaemic control for pregnant women with pre-existing diabetes, Cochrane Database of Systematic Reviews
- Continuous glucose monitoring systems for type 1 diabetes mellitus, Cochrane Database of Systematic Reviews
- Momordica charantia for type 2 diabetes mellitus, Cochrane Database of Systematic Reviews
- Interventions for pregnant women with hyperglycaemia not meeting gestational diabetes and type 2 diabetes diagnostic criteria, Cochrane Database of Systematic Reviews
- Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin, Cochrane Database of Systematic Reviews
- Saxagliptin (Onglyza) – type 2 diabetes mellitus, All Wales Medicines Strategy Group
- Type 2 diabetes: newer medicines and insulin analogues, WeMeReC
- Exenatide – Type 2 diabetes mellitus, Canadian Agency for Drugs and Technologies in Health – Common Drug Review
- Reno-protective effects of renin-angiotensin system blockade in type 2 diabetic patients: a systematic review and network meta-analysis, DARE
- Type 2 diabetes – reducing cardiovascular risk, National Prescribing Service Limited (Australia)
- Empagliflozin for type 2 diabetes mellitus, Health Technology Assessment (HTA) Database
- Review finds little evidence for Complementary and Alternative Medicines in diabetes, The Diabetes Elf
- Review: insulin pumps may improve quality of life and glycaemic control in adults with type 1 diabetes, The Diabetes Elf
- Peri-operative diabetes management guidelines, Clinical Practice Guidelines Portal, Australia
- Linagliptin rejected by the NHS in Wales for use in type 2 diabetes due to lack of evidence of efficacy, The Diabetes Elf
- Moderate physical activity is associated with lower mortality in people with diabetes, The Diabetes Elf
- Diabetes accounted for 8.9% of prescribing costs in NHS England in 2011/12, The Diabetes Elf
- Better evidence needed on the effectiveness of tailored interventions on self-management type 2 diabetes, The Diabetes Elf
- Review: more evidence needed for metformin in children with type 2 diabetes, The Diabetes Elf
- New guidelines for the management of diabetic retinopathy, The Diabetes Elf
- Review finds weak evidence favouring moderate blood sugar targets in diabetic women during pregnancy, The Diabetes Elf
- Intensive blood pressure control prevents strokes in diabetic patients with hypertension, The Diabetes Elf
- Eating disorders are common and problematic in adolescents with type 1 diabetes, The Diabetes Elf
- Review: children and adolescents with type 1 diabetes can have the same quality of life as those without it, The Diabetes Elf
- Welsh NHS recommends saxagliptin as an option in type 2 diabete, The Diabetes Elf
- Comparison of Two Creatinine-Based Estimating Equations in Predicting All-Cause and Cardiovascular Mortality in Patients With Type 2 Diabetes, Diabetes Care (EvidenceUpdates)
- Concentration of Cystatin C and Risk of End-Stage Renal Disease in Diabetes, Diabetes Care (EvidenceUpdates)
- Maternal Efficacy and Safety Outcomes in a Randomized, Controlled Trial Comparing Insulin Detemir With NPH Insulin in 310 Pregnant Women With Type 1 Diabetes, Diabetes Care (EvidenceUpdates)
- Intervention Costs and Cost-Effectiveness of a Successful Telephonic Intervention to Promote Diabetes Control, Diabetes Care (EvidenceUpdates)
- Short-term continuous glucose monitoring: effects on glucose and treatment satisfaction in patients with type 1 diabetes mellitus; a randomized controlled trial, Int J Clin Pract (EvidenceUpdates)
- Diabetic neuropathy: clinical manifestations and current treatments, Lancet Neurol (EvidenceUpdates)
- Hemoglobin A1c Versus Oral Glucose Tolerance Test in Postpartum Diabetes Screening, Diabetes Care (EvidenceUpdates)
- Combined intensive blood pressure and glycemic control does not produce an additive benefit on microvascular outcomes in type 2 diabetic patients, Kidney Int (EvidenceUpdates)
- Curcumin Extract for Prevention of Type 2 Diabetes, Diabetes Care (EvidenceUpdates)
- The cost-effectiveness of substituting physicians with diabetes nurse specialists: a randomized controlled trial with 2-year follow-up, J Adv Nurs (EvidenceUpdates)
- Performance of HbA1c as an Early Diagnostic Indicator of Type 1 Diabetes in Children and Youth, Diabetes Care (EvidenceUpdates)
A great collection of evidence. As I’ve not used it for a while, I used Wordle to create this word cloud (click to make bigger):
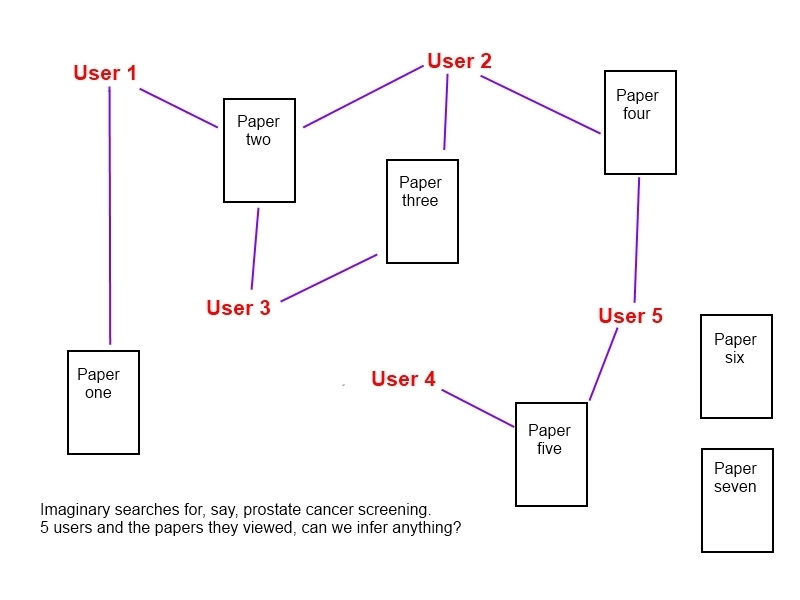
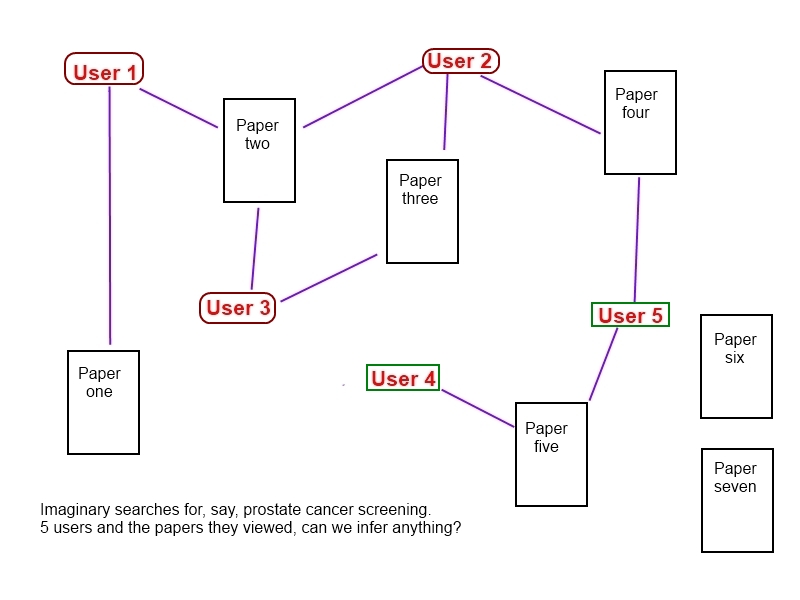
But what’s the best way of Trip using this data, not just for diabetes, what about hypertension, acne, hay fever? We want to find a great way of highlighting new evidence. It needs to look good and make people want to engage with it…! Carl highlighted what the BMJ are doing with their portals e.g. diabetes portal, not as something to aspire to but an example of one approach.
If you’ve ever seen Flipboard for iPad, I like that approach but no idea if it’d work. It might be that we use our – soon to be released – timeline. But if anyone has any ideas – please let me know.

Recent Comments