I’m not sure how many of these ‘the future of Trip’ articles I’ve written over the years, but there have been a few. I like to set out my current thinking of the direction of Trip with some reflections on the past.
Business model – our move to a freemium business model last year (most of the site free but a ‘pro’ section for those willing to pay for extra content and functionality) has been a great success. For years we have been concerned about the financial security of Trip and this new approach has allowed us to diversify our income streams and bring the security we craved!
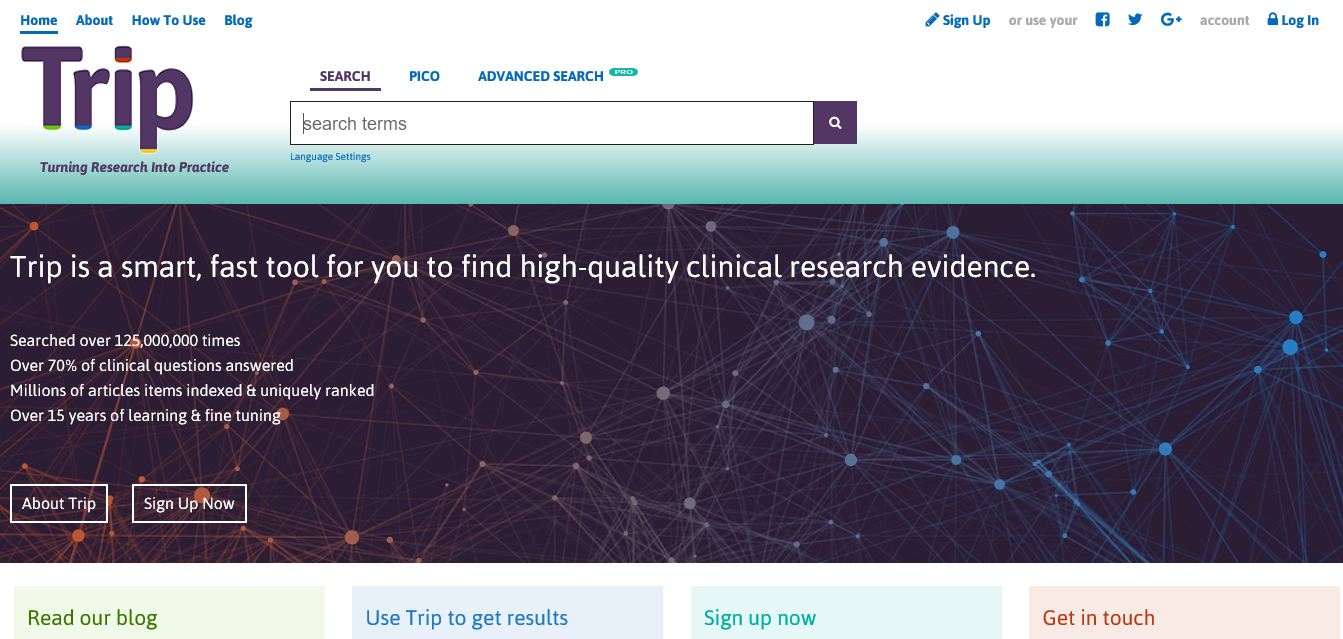
New Design – It’s been out for a few weeks now and I’m loving it and the reaction. We rolled out a few new features but it was more cleaning up the interface. It was a major piece of work and it’s great that this particular project has finished.
Answer engine – This has been talked about for years and it’ll finally be here shortly. It’ll be a learning system to give answers as well as search results.
As all this has been going on as I’ve been reading the very interesting ‘Business for Punks‘ which is an overview of the rise of the Scottish brewery Brewdog. It’s refreshing and has given me the inspiration to write this post. One big factor in their success has been the relationship with their customers, in effect, being their brand ambassadors – helping promote the business and the brand. To a large extent this happens with Trip. We have lots of fans and a great connection and I can always rely on our registered users to help out when I need advice. But one thing that Brewdog have shown is that you cannot do enough customer/user engagement. So, I’m hoping to reflect on better ways of making the Trip users feel part of Trip.
But another really powerful message is to properly define what you’re trying to do and really focus on making that magical. This is something I’ve been pondering for a while and this book helped crystallize my thinking:
What is Trip about?
Trip started as a service to my work answering clinical questions for general practitioners in Gwent, South Wales in 1997. Q&A is my passion. When we ask users about Trip we get three main reasons for using the site:
- Clinicians seeking answers to their clinical questions.
- Information specialists carrying out literature reviews for systematic reviews, guidelines etc.
- Academics using the site to plan research.
The focus of Trip developments has always been the top reason (Q&A) but I’ve been keen to support the other two. I think this will always be the case. But I do think I may have lost sight of what the Q&A component means. What do I want the site to do, in relation to Q&A? A few alternatives:
The best place for health professionals to obtain answers to their clinical questions
or
Clinical question answering heaven
or
The ‘go to’ place for clinical question answering
They all amount, roughly, to the same thing. The top one answers it best albeit being a bit wordy (but we can work on that). So, the plans for the next major developments involve supporting clinical question answering! This requires a number of components:
Answer engine – as mentioned above it’ll be rolled out soon. It won’t be perfect but it’s a great start and it’s a learning system so it’ll get better with time.
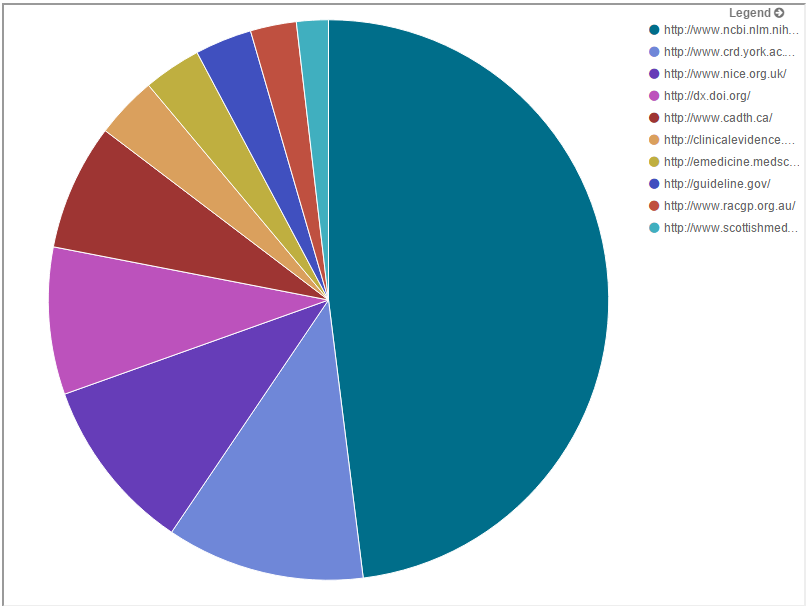
Search algorithm – we’ve followed the same basic algorithm for years, arranging results based on a mixture of word matching (between search term(s) and documents in the Trip index), year of publication and quality of the publisher. This is fine, to a point, but search has moved on massively and we’ve not moved with the times. So, we will be looking to overhaul this. As part of my work in the KConnect I will be working with information retrieval experts to exploit current ‘best practice’.
Belief – Underlying the changing has to be a belief that we can be the best.
Community – Trip needs to state our aim to be the best and to actually be the best. This will rely on our community of users letting us know when we’re great and when we’re less than great. So, our engagement with users needs to be enhanced – from good to great.
So, Trip’s future:
Community and site moving closer together to deliver something magical






Recent Comments